I would like to share with you briefly and as pleasantly as possible the daily life of someone who works in a movement analysis laboratory and how the results obtained can improve the quality of life of patients.
From the time of Aristotle to Honoré de Balzac, with his Theory of Gait, human walking was already being analyzed with the naked eye, without complex apparatus (what we understand by “complex”) or in specific places for its study. However, today a movement analysis laboratory is essential for the rigorous study of gait.
And what is a movement analysis laboratory?
Although the name already indicates what is going to be done there, let’s not leave everything to the imagination. Both the lab I work in on-site in Madrid and the one I was in during a research stay in Dublin share several common elements:
● A walking corridor or walkway.
● Some markers or sensors that are placed on the subject.
● Cameras that capture the movements of the markers; i.e., the subject.
A force platform (optional).
With these elements it is possible to reconstruct what would be a gait analysis, which, simply explained, consists of the following: after starting a recruitment phase (beware that it has to be approved by an ethics committee!) a healthy person or a patient diagnosed with a neurological disease arrives, a series of anatomical measurements of the trunk and lower limbs are taken and the markers are placed. The patient is then asked to walk along the gait walkway while his or her movement is recorded and step force information is collected via the platform interspersed in the gait walkway. After a few back and forth, the test is completed and data analysis begins.
Actually, we can skip the data analysis part.
So what do we get out of all these walks?
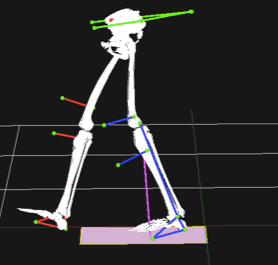
Well, two big data sets: kinematics and kinetics of the hip, knee and ankle. Kinematics refers to joint angles; knee flexion and extension, hip rotation, etc., while kinetics covers forces and their derivatives (joint moments and powers).
From all this information, together with the clinical data, a gait profile of a group of patients can be created; we define the ranges of the variables and the gait patterns of the specific group. This allows us to perform comparative analysis between the different study groups, for example HEALTHY vs. SICK or TREATMENT A vs. Information is power and even more so when the number of patients is high. The larger the sample size, the greater the statistical power of the tests we apply.
And as a final practical example, I will summarize what we have been investigating over the last year. There is a condition called idiopathic toe walking that mainly affects young children and causes a gait disturbance that causes them to walk on tiptoe. Nowadays, its diagnosis is made by exclusion of other neurological conditions in which gait is altered, such as cerebral palsy, until it finally falls under the term idiopathic. With the idea of facilitating the differentiation between idiopathic gait and other neurological diseases, pointing in the direction of early diagnosis, we decided to study gait information with one of the most powerful classification tools: Deep Learning. The interim results are promising as we are able to distinguish with more than 90% accuracy, both between the patient groups and the control group.
Can you help us to become more? Become a member and participate. Spread our word on the networks. Contact us and tell us about yourself and your project.
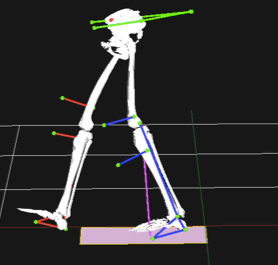
Movement Model
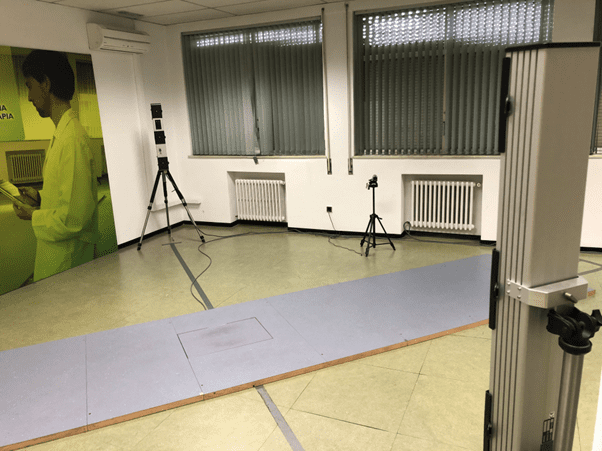
Laboratory
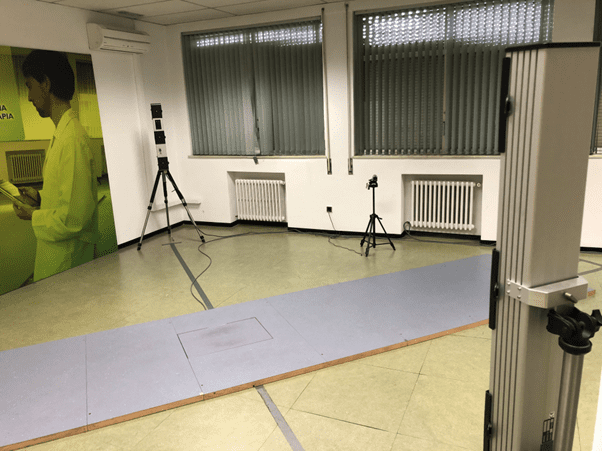
Laboratory

Alfonso de Gorostegui
PhD Candidate in Neuroscience
Hola! Mi nombre es Alfonso de Gorostegui y estoy en camino de terminar mi doctorado en Neurociencia con la Universidad Autónoma de Madrid, en concreto en el estudio de marcha de pacientes con enfermedades neurológicas.